

Laser in hemorrhoid treatment: A novel, safe and promising approach
Hemorrhoidal disease is ranked number one among colorectal diseases. Normally there are three hemorrhoid plexus in humans. These plexuses are normal part of the anal canal and have two main functions, they protect the mucosa of anal canal and prevent incontinence by closing the anal canal during rest.
When these veins become dilated they turn to a morbid condition called hemorrhoidal disease, which affects more than 80% of the world population at least once in a lifetime. Straining promotes the congestion of these veins and speeds the development of the hemorrhoids; heredity also plays an important role and it is common to observe many cases in a same family. Pregnancy, weightlifting, and anything that increases intra-abdominal pressure contributes to vein dilation.
There have been described three types of hemorrhoids, the internal, the external and the mixed. Internal hemorrhoidal disease in general is divided in four grades.
Most specialists suggest that hemorrhoid disease grade I and II should be treated initially by conservative means, and operative means should be applied only in case of recurrence or failure to control the symptoms. On the other hand, in grade III to IV the treatment should be operative.
The most common procedures during the past 60 years used to be the open hemorrhoid removal and the closed hemorrhoidal dissection that are recognised worldwide.
Many methods have focused on curing hemorrhoids including rubber band ligation, sclerotherapy, cryosurgery, laser photocoagulation, and stapled hemorrhoidopexy, doppler-guided artery ligation, depending on the severity of the disease.
The use of laser began in the 1960s, when the Nd:YAG laser was first used for anorectal surgery. The energy of the Nd-YAG laser can penetrate water and be absorbed by the tissue, inducing a thermal effect which damages the tissue, and then the effect of photocoagulation is achieved.
After that, the CO2 laser was used for laser hemorrhoidectomy was performed using a carbon dioxide laser. The method of laser hemorrhoidectomy is similar to the procedure described by Milligan and Morgan except that all dissection and hemostasis is provided by the defocused CO2 laser.
The most common techniques for hemorrhoid disease laser treatment are the HeLP technique, the LHP technique and recently the novel LSH technique or ELITE technique.
In HeLP technique a Doppler probe is used to identify the main hemorrhoidal vessel and then laser beam energy is applied to thrombose the vessel. Finally, after few days the hemorrhoid pile shrinks as a result of the blood blow stop caused by the external laser energy application.
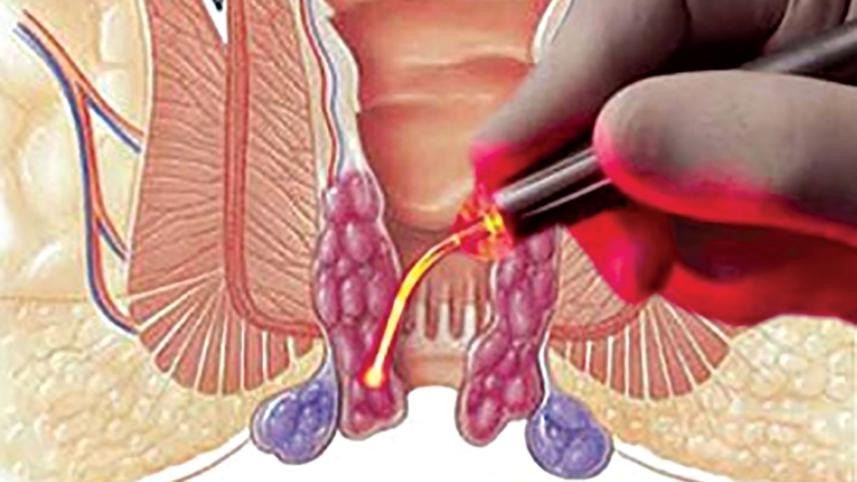
Intrahemorrhoidal laser coagulation or laser haemorrhoidoplasty was first described in 2007 and 2009 is one of the newer innovations in the management of haemorrhoidal disease. The principle of this minimally invasive technique is the coagulation of the haemorrhoidal plexus through the submucosal application of laser energy.
Recently the novel LSH technique or ELITE technique uses a special probe, containing a bare fiber within a special conical glass tip, ensuring a gentle application of laser energy.
In Bangladesh, many colorectal surgeons practise the use of Laser in the treatment of hemorrhoid. Most of the surgeons apply laser energy on three point (surface, submucosa and intrahemorrhoidal) of a single hemorrhoid, to get an effective outcome and so far the personal experience is satisfactory.
The existing data suggest that diode laser is a safe, painless and efficient alternative for the treatment of hemorrhoids, although there are still enough to be clarified. More perspectives, well organised studies with longer follow up are required to demonstrate the exact advantages of these techniques and especially to define the recurrence rate.
The writer is a Professor of Surgery at Universal Medical College & Hospital.
 For all latest news, follow The Daily Star's Google News channel.
For all latest news, follow The Daily Star's Google News channel.
Comments